

Chapter 3: The Healthcare Coalition during Emergency Response and Recovery: Concept of Operations
3.1 Establishing Procedures for the Progressive Stages of Response and Recovery
Many emergency response organizations have found it useful to conceptualize incident response and recovery in distinct stages that occur sequentially as an incident evolves. By grouping activities that have a common purpose, these stages provide a framework for the response organization's "Concept of Operations" (i.e., how the components of the response system function and interact through the successive stages of emergency response and recovery). This approach helps ensure that emergency response guidance is well organized and sequenced through specific intervals in the evolution of an incident.
Although the stages used by organizations may vary, they generally entail the same broad categorization of activities. Healthcare planners developing a Healthcare Coalition are encouraged to examine the stages presented here within the context of their own situations when they are developing the Coalition's Concept of Operations. It is also helpful to examine the planned actions of individual healthcare organizations (Tier 1) and appropriate jurisdictional entities (Tier 3) during these stages of emergency response and recovery.
The following general stages of emergency response and recovery are presented for consideration, along with the critical actions that the Healthcare Coalition should consider in each stage. By examining response actions in this manner, a comprehensive Concept of Operations for the Healthcare Coalition's Emergency Operations Plan (EOP) can be developed. These stages typically have significant overlap in their actual time of occurrence, especially early in emergency response (Figure 3-1).
Stage 1: Incident recognition. This is the interval when an organization determines whether emergency response actions are needed. The incident recognition process identifies an anomaly (either independently or through communication with others), develops a rapid situation assessment, and determines whether a response by the organization may be necessary. An "incident" exists for the Healthcare Coalition whenever an actual or potential need arises to provide emergency-related support to healthcare organizations.
Figure 3-1. Stages of incident response and early recovery
Figure 3-1 depicts the Stages of incident response and early recovery. They are, from top to bottom: Incident Recognition; Notification and Activation; Mobilization; Incident Operations; Demobilization; Transition to Recovery and Return to Readiness.
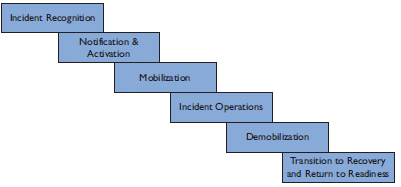
Stage 2: Initial notification/activation. Initial notification and activation occur in a relatively simultaneous fashion. "Notification" refers to the actions required to inform appropriate organizations within the response system about the onset of an incident or an important change in incident parameters. Notification conveys important details (if available) and may indicate whether the notified organizations should undertake response actions. An initial notification message accomplishes the following:
Provides urgent information about a hazard occurrence or threat of a hazard occurrence
Commonly suggests actionable guidance for the notified entity for protective and initial response actions
Conveys the activation decision regarding the HCRT.
"Activation" refers to determining the response level for the system. As applied to the Healthcare Coalition, activation refers to the decision to transition from baseline operations to HCRT operations with a designated staffing level as described in the Coalition's EOP. Activation levels may be partial or full (see Section 3.3.1). It is important to note that an activation order is binding only for personnel designated to staff the HCRT and does not require (but may request) individual member organizations to activate their emergency response procedures. Each organization determines its response actions independently based on information received through the Coalition and other sources
Stage 3: Mobilization. This refers to the transition of the HCRT from a state of inactivity or baseline operations to the designated response level.[32] Each Coalition member organization mobilizes its own response (based on its EOP) independent of the HCRT activation. Coalition members are only required to make available an Organizational Liaison to interface with the HCRT and this activity may be performed by each member organization's Liaison Officer in their activated IMT.
Stage 4: Incident operations. This stage refers to all actions that address the Healthcare Coalition's response objectives following activation of the Coalition's EOP (other than mobilization and demobilization). Actions in this stage may be divided into "initial" (or "immediate") and "on-going" categories.
Stage 5: Demobilization. This stage addresses the transition of resources, and eventually the HCRT itself, from response activities back to baseline operations. Demobilization procedures are triggered as response objectives are achieved and resources are relieved of incident responsibilities.
Stage 6: Transition to recovery and return to readiness. This stage encompasses the Healthcare Coalition's recovery activities and actions that return the Coalition to a state of readiness for the next emergency.
If the Healthcare Coalition's EOP is written to be "all-hazards," then many of the processes and procedures will be applicable regardless of the type of emergency or the response assets that are used (see Exhibit 3-1). Personnel developing a Healthcare Coalition should focus first on all-hazards processes before addressing hazard-specific issues.
Exhibit 3-1. Example of an "all-hazards" response process
A critical response action in any emergency is to document the structure of the team that is managing the incident for the organization. The team's structure should be clearly understood both internally and by external entities that must interact with the team. Documenting and disseminating the names of staff who are assigned to specific positions on the team is important, even if the organizational structure is rather simple.
The remainder of this chapter describes the actions that the Healthcare Coalition should consider in each stage of emergency response and recovery.
3.2 Incident Recognition
The ability to recognize circumstances that may indicate the need for emergency response has importance not only for the Healthcare Coalition, but for individual organizations as well. Optimal recognition of the need to activate the HCRT and determine the earliest possible and appropriate response actions may be the most important factor in a successful outcome. A specific process for incident recognition and supporting procedures should be established.
As discussed in Chapter 1, a situation becomes an "incident" for a healthcare organization when it requires the organization to activate its EOP. Activation of response systems by public health and medicine is commonly delayed due to narrow incident definitions based on casualty numbers. There are many situations in which few or no incident patients can be expected and yet activation of the EOP is warranted (e.g., utility disruption or other challenges to continuity of operations). Although it is important, the casualty count is not the sole indicator of the severity of issues that healthcare organizations will face during an incident.
In determining whether response action is warranted for the HCRT, it is important to remember that the Coalition's response is scalable. Initial incident parameters may not warrant a full activation, but partial activation may be enough to address the anticipated response functions. With this concept integrated into Healthcare Coalition procedures, early activation will have only limited cost and minimal operational impact. Thus, more frequent activations of the Coalition are justifiable in anticipating potential support needs of healthcare organizations.
Provided below is general guidance on whether a situation is an incident for a Healthcare Coalition. Each Healthcare Coalition should develop its own specific guidance based on its situation.
Activation of a healthcare organization (Tier 1): Almost any declared incident (and subsequent EOP activation) for a Healthcare Coalition member organization is, by default, an incident for the Coalition. Although the affected organization may not immediately request assistance, the Healthcare Coalition should consider partial activation of the HCRT to promote situational awareness and to be ready to assist as needed.
Activation of a Jurisdictional Agency (Tier 3): The activation of a Jurisdictional Agency's EOP may indicate the need for activation of the HCRT. The Healthcare Coalition Notification Center Technician should notify the Coalition's Duty Officer to determine whether the HCRT should be activated. Even when an incident will not likely have a major impact on individual healthcare organizations, there is often merit in providing advisories or alerts to the Healthcare Coalition. For example, if the Jurisdictional Agency activates its EOP for a brush fire, an "alert" may be issued to healthcare organizations. This promotes readiness to rapidly transition into more robust operations, if needed.
Activation of a nearby Healthcare Coalition: In regions where multiple Healthcare Coalitions exist, activation of the EOP by one Coalition may suggest partial activation by less directly impacted Coalitions. This will enable the neighboring Coalition to maintain situational awareness for its healthcare organizations and anticipate requests for assistance.
Additional criteria for considering Healthcare Coalition activation include the following:
If the Jurisdictional Agency (Tier 3) requests activation of the HCRT
If there is evidence that incident circumstances could expand, especially in an intentional situation, such as terrorism, or if incident details are unclear
If a similar incident in the past required activation of the HCRT
If the Coalition's Senior Policy Group requests HCRT activation.
To determine whether an incident exists for a Healthcare Coalition, the Coalition needs a method to be alerted about an anomaly, gather information, and conduct a balanced decision-making process. Decision makers should have well defined, incremental activation options. They should not be constrained to an "all-or-none" decision tool, which can be detrimental to timely incident recognition. Exhibit 3-2 provides several considerations for the Healthcare Coalition.
Exhibit 3-2. Healthcare Coalition Incident Recognition
To simplify decision-making processes, the Healthcare Coalition may establish two categories for initial incident information:
Incident details that clearly indicate the need for notifications to Coalition member organizations and/or activation of the HCRT. Large-scale, sudden onset incidents, such as earthquakes, transportation accidents, or terrorist attacks qualify as potential incidents that warrant notifications to Coalition members and activation of the HCRT, even if only limited initial information is available. The Coalition may establish a list of incident types to facilitate decision-making processes.
Requests from certain entities, such as a local or State Public Health department, may warrant notifications to Coalition member organizations and activation of the HCRT.
Incident information that does not clearly indicate the need for notifications to Coalition member organizations or activation of the HCRT.
A process should be established for making decisions under these circumstances. For example, the information may be vetted by the Coalition Duty Officer to determine whether a notification should be sent out and what it should include. Alternatively, the Duty Officer could attempt to obtain more information to determine next steps.
The Healthcare Coalition should strive to maintain a low threshold for recognizing anomalies as "incidents" for the Coalition. Early recognition has critical implications for the remaining stages of incident response. A low threshold is defensible if it triggers only a low-impact, limited HCRT activation until more information is known.
There are many sources that can provide relevant information to help determine whether an incident exists for the Coalition. Connectivity to these sources, which are highlighted below, should be addressed during preparedness planning to ensure the Coalition's ability to rapidly share information.
Individual healthcare organizations (Tier 1) may provide initial information indicating the need for HCRT activation.
Jurisdictional authorities (Tier 3), such as Fire, EMS, Emergency Management, Law Enforcement, and Public Health may have critical information for healthcare organizations during the early stages of an incident.
Other public sector entities, including State or Federal agencies (Tiers 4 and 6, respectively), may provide relevant information (e.g., public health advisory) to the Healthcare Coalition. This is often (but not always) communicated to the Coalition through the appropriate jurisdictional authorities (Tier 3).
Other regional Healthcare Coalitions may share information about an evolving hazard, such as an infectious disease, that prompts incident recognition.
Media may broadcast information that helps the Coalition Duty Officer decide whether to activate the HCRT. Information verification is critical when media reports are used for decision-making.
Utility services providers (e.g., water, electricity, gas) may be a valuable source of information about a hazard impact and the extent and projected length of a utility outage.
Alarm systems that exist in some regions may warn of the possibility of an actual or impending hazard impact. Examples include weather warning systems, flash flood warning systems, and environmental surveillance systems such as Bio-Watch.[33] Having specific points of contact available to the Coalition and established reporting mechanisms is critical to timely incident recognition.
3.3 Initial Notification/Activation
Once it is determined that an incident exists for the Healthcare Coalition, initial notifications must be made and the appropriate level of activation for the HCRT should be determined. These steps occur almost simultaneously, so initial notification/activation is presented here as a single response "stage."
The decision to activate the HCRT may best reside with the Coalition Duty Officer, with the authority having been conferred by the Coalition member organizations. The initial HCRT activation level may range from a single staffed position (HCRT Leader) to the staffing of all positions in the HCRT. Activation of the HCRT Leader position is differentiated from the baseline Duty Officer position by increased liaison activity between the HCRT and Coalition member organizations (Exhibit 3-3), as well as additional responsibilities.
Exhibit 3-3. Example of incident recognition and activation of the HCRT for an anticipated need
In late summer 2008, a long-term care facility in Washington, D.C. experienced a failure of its HVAC system on a warm day. It was unclear when repairs could be made and so the long-term care facility notified the Washington, D.C. Emergency Healthcare Coalition Duty Officer. An "alert" message was sent to Coalition member organizations, and the HCRT was activated with only the HCRT Leader and organizational liaison positions staffed. Coalition members were canvassed for possible bed availability in case patient evacuation was initiated at the impacted facility. Bed numbers were aggregated by location and bed-type, formatted, and provided to the affected organization. Multiple situation updates were provided to Coalition members before, fortunately, the HVAC repairs were completed. Evacuation was not necessary, and the HCRT demobilized.
Activation of the Healthcare Coalition requires rapidly staffing the designated HCRT positions. It begins with the Coalition Duty Officer either transitioning to the HCRT Leader position, or assigning another qualified individual for that role. The HCRT Leader designates which HCRT positions should be initially staffed based on the parameters of the incident. Activation messages to the personnel designated for these positions can occur in multiple ways but may best be handled via the Coalition Notification Center.
Pre-established HCRT activation levels, with the HCRT positions required for each level, may expedite the decision process. Candidate activation levels for the HCRT are:
Partial HCRT Activation: This entails minimal staffing of the HCRT at a pre-established level, but is less robust than a "full" activation. It may include activation of only a single position within the HCRT (HCRT Leader, see Exhibit 3-3).
Full HCRT Activation: Personnel are assigned to all defined HCRT positions. Because the Coalition's response is scalable, the HCRT may initially activate only a single position and rapidly scale to full activation as specific response needs are identified. Conversely, an initial full activation of the HCRT may be scaled back if the situation is less complex than first indicated.
HCRT Alert: This level requires no specific response actions by notified personnel. The requested activity could be as simple as monitoring an incident for further developments and ensuring availability for immediate activation, if indicated. In this way, a more rapid activation can be accomplished. In addition, some limited contingency planning could be conducted by the Duty Officer in case the situation evolves.
Notification messages provide information about the situation, describe current Coalition actions, such as HCRT activation, and include recommended or requested actions on the part of the notified entity.
Notification is best conducted when using pre-established urgency categories and message templates. The message should convey the relative importance of the situation and specify the need for any relevant response actions on the part of the recipient. Exhibit 3-4 presents sample categories for notification messages to Coalition member organizations. This specific categorization is also used by Federal and other response agencies. It is most important, however, that the Coalition consider using categories that are consistent with its local jurisdictional authorities (Tier 3) and its member organizations (Tier 1).
Exhibit 3-4. Sample notification categories for information provided to Coalition member organizations.
Advisory: Provides urgent information about an unusual occurrence or threat of an occurrence, but no action by the message recipient is expected. An advisory may include actionable information for individual personnel at Coalition member organizations even though the organizations may not need to take emergency action (e.g., a weather advisory that includes travel precautions for individuals).
Alert: Provides urgent information and indicates that some response action on the part of the message recipient may be necessary. An alert may also be used to notify Coalition member organizations that the HCRT has been activated. This category may also be used for ongoing notification during an emergency to convey urgent information and recommended actions from the HCRT or incident command authorities.
Update: Provides non-urgent incident information and suggests no urgent actions. This category is used in both emergency and non-emergency times (e.g., notification of a preparedness meeting may be sent as a Coalition update message.)
Adapted from Barbera JA, Macintyre AG, Shaw G, et al, Emergency Management Principles and Practices for Healthcare Systems. Department of Veterans Affairs, Veterans Health Administration (2006).
The recipients of initial and follow-on notifications can be easily pre-identified and categorized into call groups. During any HCRT activation, the following should receive an initial notification message:
Personnel expected to staff the HCRT or who are placed on standby status.
Coalition members (Tier 1) should be notified of any HCRT activation through an Alert message, even if there is no request for information from them. The Alert message should request that each member organization designate a liaison to be a point of contact for the HCRT (i.e., the Organizational Liaison). The liaison monitors HCRT messages and responds to any information requests. Healthcare organizations are responsible for disseminating these notifications within their own institution.
Jurisdictional authorities (Tier 3) should also be notified when the HCRT is activated. This helps integrate the Coalition's response with the larger community response and may provide Tier 3 entities with critical information they don't already possess. Methods for notifying Jurisdictional Agencies (Tier 3) should be established during preparedness and accomplished through a single point of contact (e.g., jurisdictional EOC, Dispatch Center, or Department of Health Operations Center). Because not all communities have well integrated communications between public sector entities, individual notification to specific entities may be required.
Other regional Healthcare Coalitions should be notified if the HCRT is activated to enhance regional situational awareness.
Notification messages should be concise and provide the appropriate urgency category. Methods can be established to convey more detailed information as it becomes available, such as posting this information to a password protected web page. Important elements in the notification message include the following:
Brief description of the threat or hazard impact
Brief description of the implications of the incident for Coalition member organizations, including any projected response actions (e.g., "healthcare facilities should anticipate significant numbers of casualties")
Specific recommended actions for individual Coalition member organizations and/or HCRT staff (e.g., requests for initial information about the hazard impact on member organizations)
Request for confirmation that the message was received by the intended recipient
Indication of when the next message will be provided, if known
Time and date stamp indicating when a message was sent.
Exhibit 3-5 provides an example template and notification message that a Healthcare Coalition might send to its member organizations.
Exhibit 3-5. Example Healthcare Coalition Alert for a train derailment
"This is an Any City Healthcare Coalition Alert (3/29/09 1630 hours). Train derailment with release of hazardous materials, including chlorine gas, near intersection of Route XX and Highway YY at 1610 hours. Area residences are being evacuated. No casualties have been reported at this time. The evacuation order may extend to Happy Times Chronic Care Facility. All Coalition member organizations are asked to provide bed count in case this facility is evacuated. Situation update message anticipated at 1700. Confirm message receipt at [web site address] and provide operational status."
Appropriate technology that is fast and reliable is required to send emergency notifications. It is important that the notification message is not easily overlooked by the intended recipient or buried in similar appearing but less urgent messages. This can be a common issue when fax is used for notifications, since fax machines are rarely monitored closely during normal operations. When using text or voice messaging, the Coalition's name and the urgency level of the notification should be given at the beginning of the message to distinguish it from other messages. Another issue to consider is the truncation of messages by pager systems, since Coalition participants may have different pager vendors with varying message capability.
Available technologies for emergency notification include:
Radio systems in which receivers are always on and near permanently staffed areas
Mass text messaging systems (e.g., Health Alert Network (HAN) systems)
Reverse 911 and other mass telephone dialing with recorded voice messaging technology
Web-based messaging services that target computers that are always staffed
Mobile web receiving devices and other emerging technology.
Because initial notifications are so important, ideal solutions may combine several technologies that offer redundant capabilities. For example, an initial Alert message may be transmitted using the HAN or other messaging system that transmits messages through multiple modalities (text, email, and telephone voice message). The message may refer the recipient to a password protected web site for further information and prompt the recipient to confirm receipt of message and convey a current operational status. Any targeted individuals and organizations not confirming message receipt in a specified time period may then be contacted through alternate methods.
3.4 Mobilization
The HCRT should be operational very rapidly at the onset of an incident. The use of pre-established procedures or a mobilization checklist can expedite and prioritize the actions that are required to transition from baseline operations to HCRT activation for emergency response. Mobilization procedures should address the following:
HCRT personnel: Personnel staffing the HCRT must receive activation notification, mobilize themselves to "assemble" (even if virtually) and be briefed. Accountability is important not only from a safety and operational standpoint, but also potentially from a financial perspective (i.e., if compensation, liability coverage, and/or other benefits are included).
Senior Policy Group personnel: Even if the services of the Senior Policy Group are not immediately needed, mobilization procedures might include verifying the contact information for Senior Policy Group personnel to ensure they can be rapidly contacted, if necessary
Coalition Notification Center Technician: For a full HCRT activation, additional staffing or a change in the configuration of the Coalition Notification Center may be needed so that incident information is adequately processed and notification and other messaging can occur. Mobilization procedures for fully staffing and accessing the Coalition Notification Center should be pre-established.
Other physical locations: Any facilities that may be used for the HCRT and/or Senior Policy Group operations should have established procedures for mobilization. Meeting space may be at these locations or distributed among Coalition members, whichever is most efficient for the specific Healthcare Coalition. Mobilization considerations are presented in Exhibit 3-6.
Exhibit 3-6. Considerations for facility mobilization
If a Healthcare Coalition will utilize fixed facilities to support HCRT operations, the following should be considered when developing mobilization procedures:
Access to the facility must be available 24/7 and procedures should be in place to comply with security requirements. For example, activated HCRT personnel may need keys, access cards, or special identification badges to access the facility.
Maps to reach the facility may be important, including the designated 24- hour entry points.
The facility that is designated for HCRT operations may have a different purpose during everyday operations. Guidance for rapid conversion of the space to allow efficient HCRT operations could include instructions on set-up of the operational space.
Procedures should include the set-up of required technology and supplies to support HCRT operations (see Section 6.2.1). This may include primary and backup telephones, cellular or satellite phones, teleconference microphone/speaker systems, computers with Internet access, radios, and direct connect devices.
In some situations, power, water, and other utilities may need to be addressed for facilities that are rarely used for emergency purposes. Availability of backup electrical, water, and other support should be verified during the mobilization process.
Potential backup locations for the HCRT operations should be identified in the event that the primary location is impacted by the hazard or is otherwise unavailable.
Mobilization procedures should be documented in the Healthcare Coalition EOP and its attachments, implemented via education, training, and drills, and evaluated through exercises or after action analyses of real-world emergencies.
3.5 Incident Operations
This section describes important activities that the HCRT may conduct during incident operations. These activities are relevant to the Healthcare Coalition regardless of whether the HCRT operates from a single physical location or via a distributed network.
As noted in Chapter 2, the HCRT position that performs the ICS "Command" function is more aptly referred to as an HCRT "Leader." Key activities of this position during HCRT incident operations are described below.
Managing the Coalition's emergency response
The HCRT Leader provides oversight and maintenance of the HCRT. Even during minimal HCRT activation, it is mandatory to designate the HCRT Leader. During initial activation, the Coalition Duty Officer transitions to the HCRT Leader position until he/she is relieved by another qualified individual. It is expected that other traditional ICS Command staff positions will be unassigned during most HCRT activations. The functions of these unstaffed positions are assumed by the HCRT Leader.
Important initial management actions include the following:
Conduct an initial situation assessment.
Designate the structure of the HCRT and which positions will be staffed for the emergency. This should be documented and disseminated to Coalition member organizations, jurisdictional authorities (Tier 3), and other relevant response organizations (e.g., regional
Healthcare Coalitions). This may be accomplished using an HCRT ICS Form 207 (Figure 3-2). Because the HCRT may evolve as the incident progresses, the structure should be updated as necessary. This level of transparency is critical to integrating the HCRT with other response entities.
Establish initial objectives for the HCRT, then develop strategies and assign resources to achieve the objectives (Exhibit 3-7). Setting objectives for the HCRT, even if formal action planning is not conducted, fosters proactive team management and is important for overall response success.
Figure 3-2. Example of an HCRT ICS Form 207 Figure 3-2 shows a sample an HCRT ICS Form. This form is used to document personnel assigned to participate in the positions in the Healthcare Coalition Response Team. Initial assignments may change and this form should be updated as necessary (even within an operational period). The form contains a revision date and fields for the 1) Incident Name; 2) Date/Time Prepared; 3) Operational Period; 4) Organizational Structure; and 5) Prepared by. The organization chart is hierarchical and each box within the chart contains a space for the Position, Home Organization, and Cell/contact. The following positions are shown in the organizational structure: HCRT Leader is at the top. Below that cell are cells for HCRT Operations Section Chief, HCRT Logistics Section Chief, and HCRT Planning Section Chief. Under the HCRT Operations Section Chief is the CNC Technician and the Organizational Liaisons. Under the HCRT Logistics Section Chief is the HCRT Communications Unit.
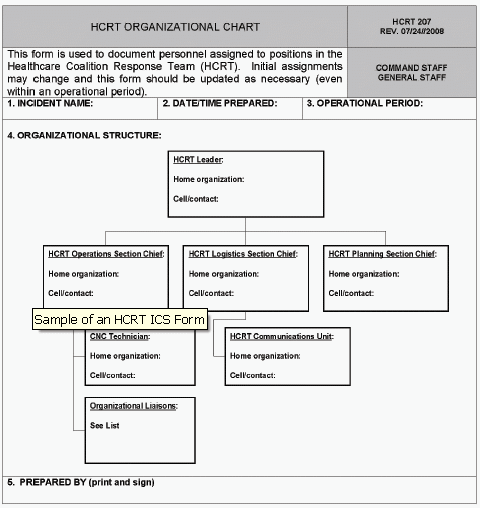
Exhibit 3-7. Example incident and initial operational period objectives for the HCRT
Incident (Control) Objectives*Facilitate situational awareness for Healthcare Coalition member organizations
Provide resource support to Coalition member organizations
Facilitate coordination across participating Coalition organizations
Facilitate the interface between jurisdictional authorities (Tier 3) and Coalition member organizations
Operational Period Objectives**
Obtain and aggregate initial situation and resource assessments at individual healthcare organizations (Tier 1)
Obtain initial situation and resource assessment from jurisdictional authorities (Tier 3) and regional sources
Facilitate early, critical requests for assistance from impacted Coalition member organizations
Obtain initial response strategies used by Coalition member organizations and assess these to identify potential conflicts or gaps
* Incident or control objective is the NIMS term for overall incident response goals and are not limited to any single operational period.
** Operational period objectives are more specific objectives (compared to incident or control objectives) for the organization to accomplish during a specific operational period, contributing towards achieving the incident objectives.Address safety issues for the Healthcare Coalition. If a Safety Officer is not assigned to the HCRT, this responsibility falls to the HCRT Leader. Safety issues for the Coalition include:
Safety issues for HCRT personnel. These will depend on the type of incident, but may include the use of Personal Protective Equipment (PPE) during a contagious disease outbreak, or addressing irregular sleep cycles for staff who are working during a prolonged incident.
Safety issues for Coalition member organizations. Collective issues related to response safety for Coalition member organizations should be addressed as well. However, this is typically addressed through the HCRT Operations Section, if established.
Address public information issues for the Healthcare Coalition. If a traditional Public Information Officer is not assigned to the HCRT, this responsibility falls to the HCRT Leader unless it is specifically assigned elsewhere (e.g., to a member of the Senior Policy Group). Public information issues for the Coalition may include:
Media inquiries about the Coalition's response during an emergency. It is important to identify an individual who can be interviewed and appropriately answer questions. Care must be taken to limit the message only to the Coalition's activities.[34] The message should not attempt to address the activities occurring at individual healthcare organizations, unless requested to do so by those assets.
Public information consistency across Coalition member organizations. The public message may need to be coordinated across healthcare organizations, if this is not specifically addressed by the relevant Jurisdictional Agency (Tier 3). This activity is best accomplished by the HCRT Operations Section (Section 3.5.2) with HCRT Leader oversight.
Conduct liaison activities. Depending on the complexity of the Healthcare Coalition and the demands of an incident, a liaison position may or may not be staffed in the HCRT during incident operations. Liaison activities, however, must still occur. An essential liaison activity is with the Jurisdictional Agency (Tier 3) or regional Jurisdictional Agencies (multiple Tier 3s). The HCRT should ensure the following:
Appropriate information exchange with the jurisdictional response. This would commonly be the Tier 3 Medical or Public Health authority through the jurisdiction's IMT, Emergency Support Function, or a Department Operations Center (e.g., Public Health Department Operations Center).
Effective interface with other regional Healthcare Coalitions (other Tier 2s), if warranted.
Interface with other response agencies that may be operating in parallel with the Jurisdictional Agency (Tier 3) that is directly supporting the Healthcare Coalition. For example, Federal Law Enforcement may be onsite at healthcare facilities to identify possible perpetrators among the incident victims. While formal interface should occur through the Jurisdictional Agency (Tier 3), direct liaison with the agency that is operating at the healthcare organization is beneficial.
Healthcare Coalition incident action planning
Incident Action Planning is an important activity for any response organization and is well described in NIMS.[35] Essentially, it is the methodology that response organizations use to proactively manage an incident by establishing incident objectives, developing strategies and tactics, and assigning resources to accomplish the objectives. It is meant to be an iterative process that continuously evaluates the success of the organization and determines whether objectives, strategies, and tactics need to be revised.
Incident action planning is often a formal process that involves a series of steps (including meetings) and documentation of the resultant action plan for dissemination.[36] Used appropriately, incident action planning can effectively coordinate the efforts of an organization and integrate those efforts with other response organizations. The following considerations related to incident action planning are relevant for the Healthcare Coalition response:
When is formal action planning indicated for the Healthcare Coalition? Despite its benefits, formal action planning can be time and labor intensive. In addition, its intra-organizational benefits are most evident to organizations conducting tactical operations (as compared to coordinating entities like EOCs). Often, an HCRT may be able to address the benefits of action planning following the response objectives set for the Coalition and simply ensuring that appropriate information is disseminated (see Section 3.5.2). If resources are available to conduct action planning, the initial incident parameters that indicate formal action planning may be beneficial include:
An incident involves or impacts a significant number of Coalition member organizations
An incident is projected to be long in duration
Incident response appears exceptionally complex, such as after a large-scale bioterrorism incident.
Moreover, if the Coalition conducts formal action planning, much of the material that is required to develop the action plan may be available by incorporating elements of the individual action plans from Coalition member organizations (Tier 1).
Who conducts formal action planning for the Healthcare Coalition? The Planning Section of the HCRT supervises the action planning process (see Section 3.5.2).
What terminology should be used for Coalition action planning efforts? Traditional ICS dictates that there is only one "Incident Action Plan" for an incident. This is usually the responsibility of the incident command authority directly managing the primary incident. The HCRT may prefer to use "Healthcare Coalition Action Plan" to distinguish this planning from both incident command authorities and planning conducted by individual healthcare organizations.
What is the scope of this formal HCRT action planning? This "Healthcare Coalition Action Plan" only addresses the scope of its activities in supporting Coalition member organizations and facilitating interface with jurisdictional authorities. To avoid confusion, the action plan should recognize activated entities such as the medical emergency support function in a local EOC or a Public Health Department Operations Center, and briefly describe how they interface.
Strategic planning and linkages to the Senior Policy Group
The HCRT Leader also manages the interface between the HCRT and the Senior Policy Group. This includes establishing a reporting cycle to provide situational awareness and HCRT performance information to the Senior Policy Group. In addition, the HCRT Leader should receive strategic or policy direction from the Senior Policy Group and supervise the implementation of the Senior Policy Group's decisions.
The organization of the HCRT Operations Section may vary based on the overall complexity of the Coalition and the specific incident requirements. Positions are staffed according to the projected tasks for that incident. The following major functions within the Operations Section are presented for consideration.
Information processing
A key response function of the HCRT could be to collect and process incident information for Coalition member organizations. The type of information processed by the HCRT may vary based upon the type and duration of an incident and by the response objectives that each Coalition seeks to achieve. It can also involve reporting the same type of information (e.g., number of incident victims by specific categories) as a response evolves. In accordance with ICS guidance, the information is captured and archived by the HCRT Planning Section.
Examples of the information categories that could be collected from Coalition organizations (Tier 1) during an incident include:
Situation reports on the operating status of healthcare organizations (Tier 1). This refers to both patient load and any hazard impact on the organization. Ideally, a template developed during preparedness will standardize information provided to the HCRT so it can be efficiently aggregated by the HCRT. The template should be somewhat flexible to capture specific information based on the incident. Common types of information that can be included in situation reports include:
The number of incident patients and types of casualties. Pre-established patient categories may be used by all Healthcare Coalition members to standardize reports on the severity of patients receiving care at each facility (Exhibit 3-8). These categories may not match up exactly with categories used by EMS to triage and prioritize patients for transport, since they serve a different purpose (i.e., projecting resource need).
Patient identifiers. This can be important for helping family members locate loved ones and for other tracking purposes (e.g., epidemiological investigation of an infectious disease outbreak). The Coalition must ensure that this information is captured in a manner that complies with relevant Health Insurance Portability and Accountability Act (HIPAA) and relevant State or local regulations.[37]
Resource reports that describe the operating status at each healthcare organization. Coalition members may be affected directly by impacts on personnel and facilities or indirectly by impacts on utilities or road access. A collective picture of the impact on healthcare delivery may offer stark evidence that priority assistance is needed through mutual aid or the Jurisdiction Agency (Tier 3). Reporting this aggregated information to incident authorities and back to Coalition members enhances situational awareness.
Exhibit 3-8. Examples of patient categorizations
The Washington, D.C. Hospital Mutual Aid System established two simple patient categories (based upon projected resource needs) for use in reporting patient data during emergencies. The simplicity works well, especially during incidents where the exact needs of the individual patients may not be rapidly discernable. All hospitals understand and utilize the following categories when reporting.
Major: patients expected to require admission and/or significant medical or hospital resources (e.g., operating room, critical care, extensive orthopedic intervention)
Minor: patients expected to be treated and released, or who require very little medical or hospital resources.
Examples of the information that could be collected from the Jurisdictional Agency(s) or other response organizations to convey to Coalition members include:
Situation reports describing the hazard impact on the community and public sector response assets.
Transportation disruptions, projected length of utility loss, EMS issues, and 911 call volumes. These are valuable data for projecting resource need and identifying barriers to resource acquisition.
Specific public health information, such as case definitions, during an infectious disease outbreak. Case definitions provided early during an incident can be critical in helping healthcare organizations collect and report epidemiological data. Rapid aggregation of these data and dissemination to Coalition members and relevant Public Health authorities may increase reporting compliance among Coalition member organizations.
Other epidemiological data collected and analyzed by public health authorities to establish situational awareness. For example, data on work absenteeism or trends in the use of specific medications can be helpful to distribute to member organizations.
Treatment protocols or guidelines promoting consistent patient care. These may be developed by expert personnel from Coalition member organizations using a consensus approach that incorporates public health recommendations. This is valuable not just for unique infectious diseases, but also when traditional medical issues must be addressed in non-traditional (alternate care) facilities. For example, general guidelines for the first 24 hours of care for burn patients who are being treated in non-burn facilities may facilitate appropriate medical care until additional assets can be mustered.
The Incident Action Plan generated by the Jurisdictional Agency (Tier 3) with command authority for the incident response. Relevant information from the Incident Action Plan should be conveyed to Coalition members, such as the projected schedule for restoring utilities or clearing debris from roadways.
Other updates, advisories, or alerts, such as an alert issued by the Centers for Disease Control and Prevention (CDC) or an "action plan" produced by a nearby Healthcare Coalition that may be dealing with a similar crisis.
What should the HCRT do with all of this information once it has been collected? This may vary from one Coalition to another, but some general next steps include:
Information provided by Coalition member organizations (Tier 1) may be aggregated or summarized into a usable format, then disseminated back to members and the relevant Jurisdictional Agency(s) (Tier 3).
The data may require some analysis to improve its value for recipients. For example, individual experts or a task force formed from within the Coalition organizations may briefly review and clarify the information before it is disseminated. Usually, the information can be distributed with minimal processing.
The HCRT Planning Section should archive all information or data collected during HCRT response and recovery.
The Operations Section can also promote situational awareness by conducting a Situation Update teleconference. This can be particularly useful during complex or rapidly evolving incidents. The objective is to provide a balanced understanding of what has occurred so healthcare organizations can make informed decisions and anticipate future actions. Participants may include HCRT personnel, Organizational Liaisons from Coalition members (Tier 1), and representatives from relevant Jurisdictional Agencies (Tier 3) and other regional Healthcare Coalitions (Tier 2s). These calls generally include an incident summary followed by short briefings from jurisdictional authorities, heavily involved Coalition members, and informed experts invited by the HCRT to participate.
Resource support
Depending on the robustness of the Coalition, another key function of the Operations Section is to facilitate resource support for responding healthcare organizations (Tier 1). It is important to note that the Coalition only facilitates the established processes for resource support. It does not direct or control these activities between member organizations or between healthcare organizations and jurisdictional response entities (Tier 3) unless specifically delegated this authority from the proper Jurisdictional Agency. Coalition actions may entail the following:
Facilitating mutual aid: The HCRT can notify Coalition member organizations when assistance is needed or anticipated by one or several Coalition members. The specific needs can be obtained from the requesting organization(s) and conveyed through the HCRT. Likewise, organizations that are able and willing to assist can respond through the HCRT so that offers of assistance can be rapidly aggregated. The HCRT can also facilitate the application of mutual aid instruments between organizations (see Chapters 4 and 7). Depending on how the Coalition has been constructed, assistance may include tracking resources shared between the organizations.[38]The HCRT must always keep Jurisdictional Agencies (Tier 3) managing the incident informed about resource requests and actions to meet the requests. Jurisdictional Agencies can then anticipate where additional assistance may be needed.
Facilitating outside assistance: Requests for assistance to entities outside of the Coalition membership can be expedited by HCRT actions. Requests from member organizations may be rapidly aggregated and transmitted to the Jurisdictional Agency (Tier 3). When a Healthcare Coalition crosses jurisdictional boundaries (e.g., the Coalition covers organizations in adjoining cities, counties, or regions), the Coalition must coordinate these requests through the respective jurisdictional authorities (Tier 3).
Facilitating requests to other regional Coalitions, whether assets are being sent to or received from these entities. Keeping relevant Jurisdictional Agency(s) informed of the situation is critical.
Facilitating the placement of specialty patients: For example, after an incident with multiple burn patients, initial care can be started at local healthcare facilities while the HCRT assists hospitals and jurisdictional authorities (Tier 3) in locating burn beds in the region, State, or country. This promotes the placement of patients via a medically sound priority scheme.
Facilitating resource support from Coalition organizations to jurisdictional authorities (Tier 3): During incidents in which the jurisdictional response entities require healthcare assistance, such as a mass biological exposure of first responders, the HCRT Operations Section can facilitate assistance from available healthcare organizations.
Facilitating a coordinated response among healthcare organizations
Certain incidents highlight the need for consistency in response actions across Coalition member organizations. This is often necessary during the response to an unusual infectious or toxic agent (evaluation and treatment protocols, case reporting, etc.). The HCRT may promote consistency across "Healthcare Organization Action Plans" by facilitating brief discussions among Coalition members and the sharing of draft action planning products as the incident evolves. Any perceived or actual conflict in the intended response actions of the organizations can then be addressed directly by the involved entities, either by producing a joint explanation for the perceived conflict or by resolving the conflicting material before it is distributed or put into action. This is a facilitating function only and does not subvert the incident command authority of Jurisdictional Agencies or the autonomy of Coalition member organizations.
Methodology
The HCRT Operations Section may establish an iterative information sharing process to facilitate coordination between the incident management elements within the responding healthcare organizations. Consistent with the ICS "management by objectives" approach, this process may entail:
An operational period (i.e., the time during which one Coalition Action Plan is applicable) is established along with a reporting schedule for Coalition member organizations.
Elements of individual organization action plans, such as patient screening protocols, may be collected and compared. Any major conflicting strategies are identified (see Exhibit 3-9).
A response coordination teleconference may be conducted. Any differences in response tactics or actions between healthcare organizations can be identified and discussed. In this manner, healthcare providers will be better prepared to address issues related to consistency in the healthcare services provided to incident patients.
An aggregated report of specific items from healthcare organization action plans may be developed. The aggregated report is forwarded to relevant Jurisdictional Agency(s) (Tier 3) while simultaneously being returned to member organizations.
Exhibit 3-9. Example of the importance of coordinating strategies of individual healthcare organizations
During the anthrax attacks in 2001, hospitals in the Washington, D.C. area did not initially coordinate their efforts for screening and evaluating potentially exposed patients. For example, some hospitals conducted nasal swabbing as a diagnostic test despite evidence that it was useful only for epidemiological purposes. The resultant confusion led to "hospital shopping" by some patients until they found a facility that would conduct the test for them. Criteria to determine which patients received prophylaxis also varied between health facilities. The lack of a consistent approach further increased the anxiety of the public and led to speculation of "class disparities" in evaluation and treatment recommendations.Authors' observations; Gursky E, Inglesby TV, and O'Toole T. "Anthrax 2001: Observations on the Medical and Public Health Response." Biosecurity and Bioterrorism: Biodefense Strategy, Practice, and Science, Volume 1, (2003).
The information contained in the Coalition members' action plans will help formulate the Healthcare Coalition's Action Plan. A consensus among the organizations may be reached for incident and operational period objectives, strategies, and major tactics. While specific tactics may vary somewhat at each organization, it is ideal to have general consistency across the Coalition.
If the Coalition elects not to conduct formal action planning, it may still be valuable to establish regular reporting times and data categories for member organizations in order to maintain situational awareness and strategy consistency. In addition, the Coalition may want to conduct the equivalent of an operations briefing at least once during each operational period. Updates on the incident and the HCRT's response actions can be provided. Participants should include the organizational liaisons to the HCRT and liaisons from relevant Jurisdictional Agencies (Tier 3).
Requirements
For the Healthcare Coalition to support these activities it must have the ability to effectively send and receive information from Coalition member organizations (Tier 1) and Jurisdictional Agencies (Tier 3). The HCRT should be able to link its member organizations in real-time for teleconferences, web-based information sharing, and other activities. Ideally, these communication methods should be available independent of Jurisdictional Agencies or any Coalition organization to ensure they are available to the Coalition during any type of major emergency.
If the HCRT is structured according to ICS principles, staffing of the various support functions (Logistics, Planning, Administration/Finance) may be necessary depending on the incident parameters and the robustness of the Coalition. To keep the Coalition as lean as possible, these functions should only be staffed as necessary for the specific emergency (see Section 2.3).
In many emergencies, the services of the Healthcare Coalition Senior Policy Group may not be needed. However, when their services are needed, the Senior Policy Group will typically meet via teleconferencing. These meetings should be managed by the HCRT Leader to keep them focused and concise. A record should be kept of the discussions and any directives from the proceedings should be disseminated to the Coalition member organizations.
The Coalition should define a process during preparedness planning for how the Senior Policy Group will make decisions during an emergency. Personnel staffing the Senior Policy Group should be trained and exercised on this decision process. For example, a majority vote may be adequate in most cases; however, if there are multiple organizations within the Coalition owned by one parent company, then consideration may be given to "weighted" votes to maintain fairness across the Coalition. The Senior Policy Group should have access to technical experts within the Coalition (Exhibit 3-10) to help them make informed decisions. At the invitation of the Senior Policy Group, representatives from Public Health, EMS, and other local Jurisdictional Agencies (Tier 3) may serve in an advisory capacity.
Exhibit 3-10. An example of a notional Senior Policy Group decision
During response to the intentional release of anthrax, the Strategic National Stockpile has been distributed according to pre-established protocols within the jurisdiction. However, due to the pattern of release, Hospital X has been screening more patients than the larger Hospital Y. A request for re-distributing pharmaceuticals has met resistance by some Coalition member organizations. To resolve the discord, an emergency meeting of the Senior Policy Group is conducted.
During the meeting, which is facilitated by the HCRT Leader, a decision is made to redistribute the medications based on an agreed-upon projection of need. A follow-up Senior Policy Group meeting is scheduled for further review and distribution revision, if indicated.
3.6 Demobilization
Given the important services that healthcare organizations provide, responding resources should be demobilized as soon as they are no longer needed for emergency response. The process for returning them to their day-to-day function should be expedited. Some organizations, as well as elements of the HCRT, may be demobilized while other elements are still operational. Individual organizations manage their own demobilization actions, but they should inform the HCRT of their status so that situational awareness can be maintained across the Coalition.
The HCRT should define procedures for demobilizing its resources. These procedures can be listed in a checklist and included as a tool in the Healthcare Coalition's EOP. Some examples of issues that could be included in a Coalition's demobilization checklist include the following:
Decision to demobilize: Guidelines for how the decision would be made and what factors should be considered (e.g., completion of response objectives) can be helpful.
Announcement of demobilization: As the Healthcare Coalition demobilizes elements from its response organization, it is important to formally notify Coalition members and the relevant Jurisdictional Agency(s) (Tier 3).
Transition to Healthcare Coalition baseline operations: As the HCRT Leader is demobilized, consultation and decision-making authority is transferred to the staffed Healthcare Coalition Duty Officer. The Coalition Notification Center resumes its role in baseline operations.
Resources: HCRT demobilization procedures can initiate the rehabilitation of HCRT resources used during the emergency. This is further addressed in Section 3.7.
Document preservation: Relevant incident-related documents for the HCRT should be archived, including ICS forms and documentation collected from external sources (Tier 1, regional Tier 2s, or Tier 3). These can be helpful for the HCRT After Action Report (AAR) process (see Chapter 6) and also serve as historical references.
3.7 Transition to Recovery and Return to Readiness
As the Healthcare Coalition demobilizes, important HCRT objectives may remain, such as supporting remaining recovery objectives for member organizations and returning the HCRT to a state of readiness for the next emergency.
There are additional management considerations for the Healthcare Coalition as its response to an incident draws to a close, including:
The HCRT Leader and the Planning Section Chief (if this position is staffed) should be the last positions to demobilize.
If the HCRT needs to support the recovery of member organizations or the jurisdiction, the staffed positions may vary from the HCRT response configuration. It may be more limited or staffed by different personnel than those who worked during HCRT emergency operations.
In addition to incident recovery objectives, the Coalition may find it useful to address mitigation or improvement in its response capabilities during recovery. Funding opportunities often arise after an emergency. The Coalition should be ready with targeted initiatives that will increase HCRT resiliency and/or improve its response capabilities.
The HCRT may assign personnel to assist with the Coalition's AAR process or other organizational learning activities. When the HCRT demobilizes, the supervision of the AAR process transitions to the Coalition's Emergency Management Committee (see Chapter 5).
All resources used during emergency response should be rehabilitated to their pre-response state. Rapid return to readiness of key resources, such as the Coalition Notification Center, should be a primary focus. Any facilities used by the Healthcare Coalition should be returned to their normal configuration. Durable equipment must be rehabilitated and non-durable supplies should be re-stocked. Information collected and processed by the HCRT should be appropriately archived.
Rehabilitation for personnel who conducted incident operations for the HCRT may entail the following:
Establishing a formal process for "out-processing" personnel and returning any issued equipment (e.g., radios)
Debriefing personnel as they are out-processed and use their feedback to inform the AAR process
Recognizing the efforts of personnel who staffed the HCRT and consider giving them personal time to recover before returning to their regular duties
Conducting performance evaluations for personnel who staffed HCRT positions during emergency operations.
Chapter 5 addresses funding of the Coalition's preparedness activities. The funding of response activities is approached differently. The primary cost for operating the HCRT and Senior Policy Group is usually personnel time, which is often donated by the Coalition member organizations. However, it is still important to keep records of personnel time (or other Coalition expenses), since reimbursement mechanisms may be available. In some situations, established mechanisms may exist for reimbursing Coalition expenses (Exhibit 3-11).
Exhibit 3-11: Regional Hospital Preparedness Council and the Catastrophic Medical Operations Center*
A variety of medical organizations within 18 counties of Southeast Texas have organized to develop a Coalition that addresses common emergency preparedness and response issues. The Regional Hospital Preparedness Council is a 501c3 independently chartered organization that functions as a preparedness platform for these organizations. During emergency response, the associated Catastrophic Medical Operations Center (CMOC) is staffed to address many of the response objectives listed for Coalitions in section 2.2 of this handbook. For example, as Hurricane Ike approached Texas in 2008, the CMOC facilitated patient tracking for the evacuation of 56 hospitals and 220 nursing homes over a 60-hour period.
The CMOC is organized using a NIMS-consistent Incident Management Team structure with subject matter experts covering traditional ICS functions. Additional liaisons have included representatives of agencies such as HHS, Department of Aging and Disability, EMS, and Medical Societies.
The council currently receives no direct State or Federal preparedness funding. However, when the CMOC is activated by the State or a local jurisdiction during a declared emergency or disaster, it is financially supported through contract. Funds reimburse the costs of personnel staffing the CMOC as well as specified other expenses.
*Personal communication between the author (AGM) and Lori A. Upton, RN, BSN, MS; January 28, 2009.
32 Drabek TE, Hoetmer GJ (Eds). Emergency Management: Principles and Practice for Local Government, International City Management Association, Washington, D.C.; (1991).
33 Shea DA, Lister SA. The BioWatch Program: Detection of Bioterrorism (November 19, 2003). Congressional Research Service Report No. RL 32152.
34 Global assessments of the situation are the role of the Public Information Officer from the relevant Jurisdictional Agency.
35 Department of Homeland Security, National Incident Management System (NIMS), December 18, 2008.
36 Commonly known as "ICS forms," there are numbered document templates that are used to form the basic Incident Action Plan. ICS forms 202, 203, 204, 205, and 206 form the core components of the Incident Action Plan.
37 Healthcare Coalitions may find it helpful to work closely with local and State public health authorities to formally address these concerns.
38 Resource tracking may occur at the healthcare organization level; however, the HCRT should still confirm that the resource tracking is actually occurring.