Official websites use .gov
A .gov website belongs to an official government organization in the United
States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you’ve safely
connected to the .gov website. Share sensitive information only on official, secure websites.
BARDA uses other transaction agreements (OTAs), a type of flexible, strategic partnership between the government and industry, to foster innovation and promote collaboration. OTAs help BARDA identify and attract nontraditional commercial firms or consortia to partner with the government.
Flexible portfolio-based funding: Partners can jointly decide to move candidates into and out of the portfolio based on product performance, technical risk, and programmatic need. This flexibility results in significant time, effort, and cost savings to both partners.
Consortia partnering: Non-traditional firms and the government can enter into consortia with multiple industry partners. Through consortia, companies can identify products in development by other companies that could be brought in to the portfolio through in-licensing, co-development, or alliances with other companies.
Time and cost savings: OTAs also allow the government and its industry partner(s) to decide jointly to replace an underperforming candidate in the portfolio with a promising new candidate. This flexibility results in a significant time, effort and cost savings for both partners.
Cost Sharing: BARDA may be able to provide steady, non-dilutive funding over multiple years. When licensed, the new products will become available on the commercial market, which means not only a return on investment for the company but also alleviates the need for government stockpiling, resulting in a long-term cost savings for taxpayers.
True collaboration: All partners are represented on joint scientific or technical oversight committees. BARDA brings insight about the nation's biodefense and ensures that there is a sound rationale for portfolio decisions. The committees endorse potential new projects, agree on how funding should be allocated, and evaluate overall performance.
Other Transaction for Advanced Research
An Other Transaction for Advanced Research (OTAR) is the legally binding, non-acquisition instrument used to advance research and development. OTARs provide flexibilities in the application of many laws and regulations that are not typically used in the commercial sector.
OTARs can be used only if at least one of the following conditions exist:
At least one of the partners is non-traditional and is participating to a significant extent
Exceptional circumstances justify the use of an OTAR because a conventional arrangement would not be feasible.
OTARs provide flexibilities in the application of many laws and regulations that are not typically used in the commercial sector while enabling BARDA to maintain proper stewardship of federal funds. To the maximum extent practicable, cost or resource sharing of program costs between the government and the nonfederal parties is encouraged.
Laboratory biosafety describes the application of specific practices, safety equipment and specially designed laboratories to create a safe environment, both within and outside the laboratory, for work conducted with infectious agents and toxins. In addition, there is monitoring for occupationally acquired infections and staff training, as appropriate.
"Biosafety Levels" (BSLs) are designations applied to projects or activities conducted in laboratories in ascending order of containment based on the degree of the health-related risk associated with the work being conducted. In the United States, the designations BSL-1, BSL-2, BSL-3, and BSL-4 describe the minimum safe work practices, specially designed buildings, and safety equipment required to conduct work on infectious microorganisms and other biological hazards. BSL-4 is the highest biosafety level.
The appropriate BSL for a project is determined jointly by the principal investigator, the institutional biosafety professionals and biosafety committees. The BSL assigned to a project is based on a biological risk assessment that takes into account:
The nature of the infectious agent, toxin, or other biological hazard, including:
Its ability to cause disease and the way(s) in which it causes disease (transmissibility and pathogenicity);
How much of it is required to cause disease (infectious dose);
How many different organisms are susceptible to infection (host range); and
Its prevalence in the community (epidemiology);
The specific laboratory activity or activities being performed; and
The availability of preventive medical countermeasures (i.e., vaccines) or effective treatment (i.e., post-exposure vaccination and/or use of antimicrobials, antivirals and chemotherapeutic agents).
The BSL assigned to a project determines the controls required to conduct the work safely:
Engineering controls, including facility construction and design elements in the laboratory space;
Administrative controls, including specific access, training, and occupational medicine policies; and
Laboratory practices and procedures workers use when working in the laboratory.
Every biological laboratory, regardless of biosafety level, follows standard microbiological practices. Each biosafety level builds on the controls of the next lower level. Each biosafety level has its own specific containment controls. The assignment of a biosafety level to a particular work process is made through a protocol driven risk assessment.
For more information on other aspects of the biosafety levels, please see the rest of the biosafety section for a general overview.
Laboratory Containment for Human Pathogens: Biosafety Level 1 – Biosafety Level 4 Facilities
BSL-1 labs are used to study infectious agents or toxins not known to consistently cause disease in healthy adult humans or animals. Workers follow basic safety procedures, called standard microbial practices, and require no special equipment or design features. Standard engineering controls in BSL-1 laboratories include easily cleaned surfaces that are able to withstand the basic chemicals used in the laboratory.
Specific considerations for a BSL-1 laboratory include the following:
Laboratory Practices
Standard microbiological practices are followed.
Work can be performed on an open lab bench or table.
Safety Equipment
PPE (lab coats, gloves, eye protection) are worn.
Facility Construction
A sink must be available for hand washing.
The lab should have doors to separate the working space with the rest of the facility.
BSL-2 laboratories are used to study moderate-risk infectious agents or toxins that pose a moderate danger if accidentally inhaled, swallowed, or exposed to the skin. Design requirements for BSL-2 laboratories include hand washing sinks, eye washing stations, and doors that close and lock automatically. BSL-2 laboratories must also have access to equipment that can decontaminate laboratory waste, including an incinerator, an autoclave, and/or another method of decontamination, depending on the biological risk assessment.
In addition to BSL-1 considerations, BSL-2 laboratories have the following containment requirements:
Laboratory Practices
Access to the laboratory is restricted when work is being conducted.
Safety Equipment
Appropriate PPE is worn, including lab coats and gloves, eye protection and face shields.
An autoclave or an alternative method of decontamination is available.
Facility Construction
The laboratory has self-closing doors.
A sink and eyewash are readily available.
BSL-3 laboratories are used to study infectious agents or toxins that may be transmitted through the air and cause potentially lethal infections. Researchers perform all experiments in a biosafety cabinet. BSL-3 laboratories are designed to be easily decontaminated. As an additional safety measure, these laboratories must use controlled, or "directional," air flow to ensure that air flows from non-laboratory areas (such as the hallway) into laboratory areas.
Other engineered safety features include a requirement for entry through two self-closing, interlocked doors, sealed windows, floors and walls, and filtered ventilation systems. BSL-3 labs must also be equipped to decontaminate laboratory waste using an incinerator, an autoclave, and/or another method of decontamination, depending on the biological risk assessment.
In addition to BSL-2 considerations, BSL-3 laboratories have the following containment requirements:
Laboratory Practices
An Occupational Health Program exists for medical surveillance of laboratory workers. Laboratory workers are under medical surveillance and may be offered immunizations for infectious agents or toxins they work with, if available.
Access to the laboratory is restricted and controlled at all times.
Safety Equipment
Appropriate PPE must be worn, and respirators might be required.
All work with infectious agents or toxins must be performed within an appropriate biosafety cabinet.
Facility Construction
A hands-free sink and eyewash are available near the exit.
Exhaust air cannot be recirculated, and the laboratory must have sustained directional airflow by drawing air into the laboratory from clean areas towards potentially contaminated areas.
Entrance to the lab is through two self-closing and interlocked doors.
BSL-4 laboratories are used to study infectious agents or toxins that pose a high risk of aerosol-transmitted laboratory infections and life-threatening disease for which no vaccines or therapies are available. The laboratories incorporate all BSL-3 features, as well as, additional safety features. Access to BSL-4 laboratories is carefully controlled and requires significant training.
There are two types of BSL-4 laboratories:
Cabinet Laboratory: All work with infectious agents or toxins is done in a Class III Biosafety Cabinet with very carefully designed procedures to contain any potential contamination. In addition, the laboratory space is designed to also prevent contamination of other spaces.
Suit Laboratory: Laboratory personnel are required to wear full-body, air-supplied suits, which are the most sophisticated type of PPE. All personnel shower before exiting the laboratory and go through a series of procedures designed to fully decontaminate them before leaving.
While the engineering controls required for BSL-4 cabinet and BSL-4 suit laboratories differ in some respects, the controls are extensive and supplemented by carefully designed procedures and practices in both types of laboratories.
In addition to BSL-3 considerations, BSL-4 laboratories have the following containment requirements (this list is not exhaustive):
Laboratory Practices
Change clothing before entering.
Shower upon exiting.
Decontaminate all materials before exiting.
Safety Equipment
All work with infectious agents or toxins must be performed within a certified biosafety cabinet, for work performed in the cabinet laboratory, or while wearing a full body, air-supplied, positive pressure suit.
Facility Construction
The laboratory is in a separate building or in an isolated and restricted zone of the building.
The laboratory has dedicated supply and exhaust air, as well as vacuum lines and decontamination systems.
Life sciences research provides for improved health care for humans, animals, and plants; protection and response against infectious diseases; and innovation and competition in a global economy...
Industrial Base Expansion (IBx) Connect is used to coordinate specific strategic innovation and industrial base expansion efforts across ASPR, federal partners, academia and the private sector. Our goal is to work with the private sector on novel solutions and practices for response and recovery operations and bring them to life.
IBx Connect meetings are for market research purposes only and are not considered submissions for potential funding.
IBx Connect aids in market research to find innovative solutions that address vulnerabilities in our nation's public health and medical industrial base and supply chains. Of particular interest are advanced manufacturing efforts for drug substances and drug products; supply chain optimization; testing and diagnostic devices and consumables and personal protective equipment (PPE).
The IBx Connect portal serves as ASPR's single point of entry for the submission of market research packages and related meeting requests from interested stakeholders regarding products they are developing that could be used to strengthen public health and medical supply chains. Through IBx Connect, ASPR seeks information from stakeholders who are developing solutions to build and sustain a resilient medical industrial base in the U.S.
ASPR is looking for products that address one or more of the following priority areas.
Advanced Manufacturing
Advanced manufacturing technologies for drug substance and drug product manufacturing
Distributed manufacturing of drug substances and drug products
Additive manufacturing
Biologically-derived manufacturing of drug substances or drug products
Supply Chain Optimization
Last mile delivery solutions
National and global supply chain optimization tools
Tools or systems for supply chain resiliency, including grid-independent solutions
PPE Manufacturing
PPE manufacturing expansion
Novel sub-tier manufacturing capabilities
Materials science applications for PPE reuse
Innovative materials to lower costs and increase capacities.
Testing and Diagnostics Manufacturing
Testing and Diagnostic manufacturing expansion
Novel sub-tier manufacturing capabilities
Next-generation sequencing and multi-omic approaches
Antibodies/antigens
Proteins/peptides/proteomic
Metabolic/metabolomic
Predictive analytics
Next generation diagnostics for novel agents
Product Maturity
IBx Connect is seeking information about products and technologies that have achieved one or more of the following milestones:
Progressed into or beyond clinical trials
Currently being produced at scale
Utilizes an approved platform
Applying to Meet with the IBx Connect Team
If your company or organization is developing a technology or product or has one available that meets the criteria described above, request to meet with the IBx Connect Team.
IBx Connect is looking for information on a wide range of innovative products and technologies to bolster resiliency across the entire public health and medical industrial base, but ASPR is interested in the development of a range of medical countermeasures that are outside the scope of IBx Connect.
BARDA is accepting submissions regarding development of medical countermeasures to address health security threats, including drugs, vaccines, and targeted diagnostics, through MedicalCountermeasures.gov and your company can request a meeting with BARDA through TechWatch.
The Strategic National Stockpile (SNS) can provide a variety of ventilator models to supplement state, local, tribal and territorial supplies in an emergency, and each ventilator has different features and modes of ventilation.
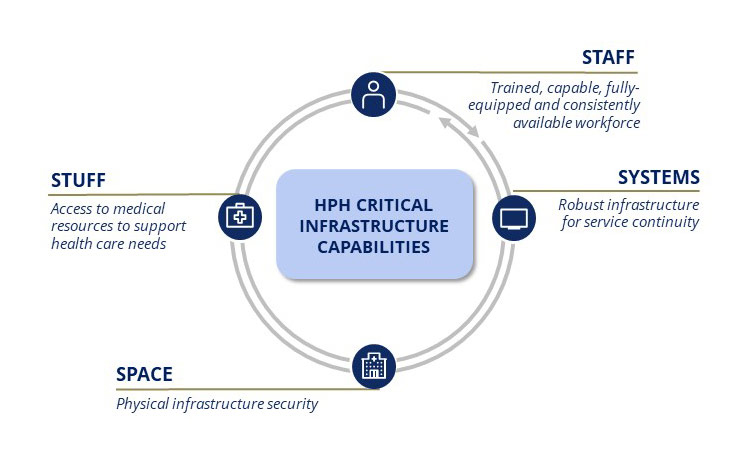
The Healthcare and Public Health (HPH) Sector is one of the 16 critical infrastructure sectors authorized by Presidential Policy Directive 21 with a mission to protect essential healthcare and public health assets and services from existential threats. The HPH Sector's activities are led by ASPR's Division of Critical Infrastructure Protection, and organized around a strong partnership between federal, state, local, tribal, and territorial (FSLTT) governments with private sector owners and operators to protect critical infrastructure, including space (e.g., facilities), staff (e.g., healthcare workers), stuff (e.g., personal protective equipment), and systems (e.g., information technology).
Since the majority of the Sector's assets are privately owned and operated, collaboration and information-sharing between the public and private sectors is essential to increasing resilience of the nation's HPH critical infrastructure. As such, under CIP's coordination and oversight, the HPH Sector convenes private sector partners across six subsectors: direct patient care, health information technology, health plans and payers, mass fatality management services, medical materials, and laboratories, blood, and pharmaceuticals with counterparts with respective equities from FSLTT partners.
Waivers or modifications may be issued to ensure that in an emergency area, during an emergency period, sufficient health care items and services are available to the maximum possible extent to meet the needs of individuals enrolled in Social Security Act (SSA) programs and that providers of such services in good faith who are unable to comply with certain statutory requirements are reimbursed and exempted from sanctions for noncompliance other than fraud or abuse.
Waivers or Modifications of Requirements
The Secretary may waive or modify certain Medicare, Medicaid, Children's Health Insurance Program (CHIP), HIPAA, and EMTALA requirements as necessary.
Requirements
Description
Conditions of Participation
certain conditions of participation, certification requirements, program participation or similar requirements for individual health care providers or types of health care providers
Pre-approval
pre-approval requirements
Licensure
requirements that physicians and other health care professionals hold licenses in the State in which they provide services if they have a license from another State (and are not affirmatively barred from practice in that State or any State in the emergency area) for purposes of Medicare, Medicaid, and CHIP reimbursement only
Sanctions
sanctions under EMTALA for redirection or reallocation of an individual to another location to receive a medical screening pursuant to an appropriate state emergency preparedness plan or a state preparedness plan for transfer of an individual not stabilized due to the declared Federal public health emergency. A waiver is effective only if actions do not discriminate based on payment source or ability to pay.
sanctions under section 1877(g) (Stark) relating to limitations on physician referral under such conditions as CMS determines appropriate.
sanctions and penalties arising from noncompliance with HIPAA privacy regulations relating to patient agreement, facility directory opt-out, notice of privacy practices, or privacy restrictions/confidential communications. Effective only if actions do not discriminate based on payment source or ability to pay.
Deadlines/Timetables
deadlines and timetables for performance of required activities to allow timing modifications
Payment limitations
limitations on payments to permit Medicare Advantage enrollees to use out-of-network providers during emergencies, with reconciliation so enrollees do not pay additional charges
Notice and Reporting
At least two days before formally exercising the waiver authority, the Secretary must provide certification and notice to Congress describing the provision waived or modified, the providers affected, geographic area, duration, and justification. A report must be submitted within one year after the emergency period ends.
Duration of Waivers and Modifications
Waivers or Modifications
Duration
Waivers or modifications
May be retroactive to the beginning of the emergency period (or later date)
Terminate upon termination of the emergency or 60 days after publication (subject to 60-day renewals)
EMTALA Waivers (non-pandemic) or HIPAA requirements
Effective only for 72 hours beginning on implementation of a hospital disaster protocol
For pandemic disease emergencies, effective until termination of the pandemic-related public health emergency
Note: A particular waiver or modification may terminate earlier if the Secretary determines it is no longer necessary.
Under section 319 of the Public Health Service (PHS) Act, the Secretary of the Department of Health and Human Services can declare a Public Health Emergency (PHE) if he determines, after consulting with such public health officials as may be necessary, that 1) a disease or disorder presents a PHE, or 2) a PHE, including significant outbreaks of infectious diseases or bioterrorist attacks, otherwise exists. A PHE declaration allows the Secretary to take certain actions in response to the PHE. In addition, a public health emergency can be a necessary step in authorizing the Secretary to take a variety of discretionary actions to respond to the PHE under the statutes HHS administers.
Questions have arisen from states, political subdivisions, and the healthcare community regarding PHE declarations. The following is not an exhaustive review of section 319 of the PHS Act or of PHE declarations in all contexts, nor a protocol for the Department of Health and Human Services' (HHS) implementation of a PHE declaration.
Under section 319 of the PHS Act, when the Secretary has declared a PHE, consistent with his other statutory authorities, he can take such action as may be appropriate to respond to the PHE including making grants; entering into contracts; and conducting and supporting investigations into the cause, treatment, or prevention of the disease or disorder. The Secretary may also, upon request of the recipient of such award and subject to corresponding reductions in payments, provide supplies, equipment, and services, and detail employees of the Department to the recipient to aid the recipient in carrying out the award. In addition, the Secretary may use funds appropriated to the Public Health Emergency Fund (when funds are appropriated to this Fund) to immediately respond to the PHE or a potential PHE by facilitating coordination among Federal, State, local, Tribal and territorial entities and public and private health care entities; making awards; supporting advanced research and development and biosurveillance; supporting initial emergency operations related to preparation and deployment of NDMS teams, and other actions determined appropriate and applicable by the Secretary. Finally, the Secretary may grant extensions or waive sanctions relating to submission of data or reports required under HHS laws, when the Secretary determines that as a result of the PHE, individuals or public or private entities are unable to comply with deadlines for such data or reports.
A PHE declaration can be a necessary step in enabling the Secretary to take a variety of discretionary actions to respond to the PHE. Certain authorities have been added to the PHS Act; the Social Security Act (SSA); and other laws administered by the Secretary that permit the Secretary to take certain actions when he has declared a PHE under section 319 of the PHS Act.
For example, the Secretary may:
Waive or modify certain Medicare, Medicaid, Children's Health Insurance Program (CHIP), and Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule requirements. Under section 1135 of the SSA, the Secretary may waive or modify certain requirements as necessary to ensure to the maximum extent feasible that, in an emergency area during an emergency period, sufficient healthcare items and services are available to meet the needs of individuals enrolled Medicare, Medicaid, and CHIP and that providers of such services in good faith who are unable to comply with certain statutory requirements are nonetheless reimbursed and exempted from sanctions for noncompliance, absent fraud or abuse. There must also be a Presidential declaration of an emergency or disaster in order to exercise this authority. See the response to items 3-6 below for details about this authority.
Adjust Medicare reimbursement for certain Part B drugs. Most Medicare Part B drugs are paid on the basis of the manufacturer's average sales price (ASP), which manufacturers are required to report quarterly. The ASP-based payment allowance is updated prospectively each quarter, using the data manufacturers report. The statutory scheme results in a two-quarter lag between the date of the reported sale and the date that sale's price is factored into the Medicare payment rate. In the case of a PHE in which there is a documented inability to access drugs and biologicals and a concomitant increase in the price of a drug or biological that is not reflected in the manufacturer's ASP for one or more quarters, the Secretary may use the wholesale acquisition cost or other reasonable measure of drug or biological price instead of the manufacturer's ASP. The substituted price or measure may be used until the price of the drug or biological has stabilized and is substantially reflected in the manufacturer's ASP.
Enable the Centers for Disease Control and Prevention Director to access the Infectious Diseases Rapid Response Reserve Fund (when funds are so appropriated) to prevent, prepare for, or respond to an infectious disease emergency, either when the Secretary has declared a public health emergency or when the Secretary determines that the emergency has significant potential to imminently occur and potential on occurrence, to affect national security or the health and security of US citizens, domestically, or internationally.
Waive certain Ryan White HIV/AIDS grant program requirements. Under section 2683 of the PHS Act, up to five percent of the funds available under each of the Parts A and B supplemental pools may be shifted to ensure access to care during the time period when the Secretary declares a PHE or when the President declares an emergency or major disaster under the Robert T. Stafford Disaster Relief and Emergency Assistance Act ("Stafford Act") or the National Emergencies Act in the geographic area where the emergency, major disaster, or PHE exists. In addition, the Secretary may waive such requirements of title XXVI of the PHS Act, which addresses health care services related to HIV infection, to improve the health and safety of those receiving care under this title and the general public. This waiver authority is limited to the time period for which the emergency, major disaster, or PHE declaration exists.
Make temporary (up to one year or the duration of the emergency) appointments of personnel to positions that directly respond to the PHE when the urgency of filling positions prohibits examining applicants through the competitive process. The Secretary may also waive dual compensation (salary offset) for temporarily re-employed annuitants during the time period when the Secretary declares a PHE or the President declares a national emergency involving a direct threat to life or property or other unusual circumstances.
Use funds from the fiscal year 2019 appropriation to HHS that are available for salaries and expenses of HHS employees to pay travel and related expenses of an employee or family member when the employee is assigned to duty in the U.S. or in a U.S. territory during a period and in a location that are the subject of a public health emergency declaration, and travel is necessary to obtain medical care for an illness, injury, or medical condition that cannot be adequately addressed in that location at that time.
Modify practice of telemedicine. The Ryan Haight Online Pharmacy Consumer Protection Act and implementing regulations allow the Secretary, with concurrence of the DEA Administrator, to designate patients, location of patients, and use of controlled substances during a public health emergency declared by the Secretary.
Enable the Secretary of Defense, in consultation with the Secretary, to deploy military trauma care providers providing care at high-acuity trauma centers pursuant to grants awarded under section 1291 of the PHS Act.
Grant an extension or waive application deadlines or compliance with any other requirement of certain SAMHSA grants, on a State by State basis, as the circumstances of the emergency reasonably require and for the period of the emergency. Such grants include those authorized under sections 521, 1911, or 1921 of the PHS Act. This authority also applies to allotments authorized under Public Law 99-319.
Allow State and local governments to access the General Services Administration (GSA) Federal supply schedule when using federal grant funds. GSA policy allows state, local, and tribal government grantees to use federal supply schedules to respond to public health emergencies declared by the Secretary. Pursuant to 48 U.S.C. § 1469e as amended, Puerto Rico, Guam, American Samoa, the Commonwealth of the Northern Mariana Islands, and the U.S. Virgin Islands may always buy off of the GSA schedules regardless of whether there is a declared PHE.
Temporary reassignment of state and local personnel. The Secretary may authorize a requesting Governor of a state or tribal organization to temporarily reassign state and local public health department or agency personnel funded in whole or in part through programs authorized under the PHS Act to immediately address a public health emergency in the state or Indian tribe during the period of the emergency.
Limit liability of health care professionals who are members of the Medical Reserve Corps or professionals included in the Emergency System for Advance Registration of Volunteer Health Professionals responding to a PHE in the initial 90 days so that such professionals shall be subject only to the State liability laws in which the professional has been deployed to respond to the PHE and only to the extent permitted under the laws of the State in which care is provided.
Determine a waiver of Paperwork Reduction Act (PRA) requirements is necessary. Section 319(f), recently added by the 21st Century Cures Act, allows the Secretary to determine that the circumstances of a PHE or a disease or disorder, including a novel and emerging public health threat that is significantly likely to become a PHE, necessitate a waiver from PRA requirements. If the Secretary makes such a determination, then PRA requirements for voluntary collection of information do not apply during the immediate investigation of, and response to the PHE during the period of the PHE or the time period necessary to determine if a disease or disorder, including a novel and emerging public health threat, will become a PHE.
Waive certain requirements of the Drug Supply Chain Security Act (DSCSA). A public health emergency is considered an "emergency medical reason" under the DSCSA, 21 U.S.C. 360eee. Thus, upon the Secretary's declaration of a public health emergency, certain activities are automatically excluded through the time period of the declaration. Notably, product distribution for such emergency medical reasons is excluded from the DSCSA definitions of "transaction" and "wholesale distribution." Therefore, the DSCSA requirements related to product tracing and wholesale distribution do not apply to trading partner activities that address the public health emergency declaration.
Allow the Department of Labor (DOL) to issue dislocated worker program grants for disaster relief employment pursuant to 29 U.S.C. § 3225. A federal agency emergency or disaster declaration or a Stafford Act declaration triggers an opportunity for eligible entities to apply for disaster relief employment National Dislocated Worker Grants. In order for a federal agency declaration to trigger this authority, the chief official of a federal agency with authority for or jurisdiction over the federal response must declare or otherwise recognize an emergency or disaster situation of national significance that could result in a potentially large loss of employment.
The Secretary may exercise his authority under section 1135 of the SSA ("1135 waiver") to temporarily waive or modify certain Medicare, Medicaid, CHIP, and HIPAA requirements in an emergency area during the emergency period. An emergency area and period is where and when there is: a) an emergency or disaster declared by the President pursuant to the National Emergencies Act or the Stafford Act, and b) a PHE declared by the Secretary.
Under section 1135 of the SSA, the following Medicare, Medicaid, CHIP, and HIPAA Privacy Rule requirements may be waived or modified:
Certain conditions of participation, certification requirements, program participation, or similar requirements for individual healthcare providers or types of health care providers, and pre-approval requirements.
Requirements that physicians and other health care professionals hold licenses in the state in which they provide services if they have a license from another state and are not affirmatively barred from practice in that state or any state in the emergency area (note however, that this waiver is for the purposes of Medicare, Medicaid, and CHIP reimbursement only – states determine whether a non-federal provider is authorized to provide services in the state without state licensure).
Sanctions under the Emergency Medical Treatment and Labor Act (EMTALA) for direction or relocation of an individual to another location to receive medical screening pursuant to an appropriate state emergency preparedness plan or a state pandemic preparedness plan or for the transfer of an individual who has not been stabilized if the transfer is necessitated by the circumstances of the declared federal public health emergency. A waiver of EMTALA sanctions is effective only if actions under the waiver do not discriminate on the basis of a patient's source of payment or ability to pay. EMTALA waivers are subject to special time limits. See question 6 for more information.
Sanctions under section 1877(g) (Stark) relating to limitations on physician referral under such conditions and in such circumstances as the Centers for Medicare & Medicaid Services (CMS) determines appropriate.
Deadlines and time tables for performance of required activities to allow timing of such deadlines to be modified.
Limitations on payments for health care items and services to permit Medicare Advantage plan enrollees to use out-of-network providers in an emergency situation. To the extent possible, the Secretary must reconcile payments so that enrollees do not pay additional charges and so that the plan pays for services included in the capitation payment.
Sanctions and penalties arising from noncompliance with HIPAA privacy regulations relating to: a) obtaining a patient's agreement to speak with family members or friends or honoring a patient's request to opt out of the facility directory; b) distributing a notice of privacy practices; or c) the patient's right to request privacy restrictions or confidential communications. The waiver of HIPAA requirements is effective only if actions under the waiver do not discriminate on the basis of a patient's source of payment or ability to pay. These HIPAA waivers under are subject to special time limits. See question 6 for more information.
No, in past practice when the Secretary has issued an 1135 waiver, the Medicare, Medicaid, and CHIP requirements that may be waived or modified under that 1135 waiver are not automatically waived or modified. Rather, CMS receives requests from affected hospitals, healthcare facilities, and healthcare providers for waivers or modifications of specific requirements and issues instructions or guidance as needed. CMS reviews such requests and generally approves the requested waivers or modifications on a case by case basis. Regardless of whether the Secretary has made a formal PHE declaration under Section 319 of the PHS Act, and even in the absence of an 1135 waiver, other SSA provisions and CMS regulations may provide certain flexibilities that may be implemented as appropriate to address an emergency or disaster. CMS works closely with affected hospitals, healthcare facilities, and healthcare providers during such situations to address their concerns.
With regard to the HIPAA sanctions and penalties that may be temporarily waived under section 1135 of the SSA, when the Secretary issues an 1135 waiver, HHS' current practice is to automatically waive such sanctions and penalties described in the 1135 waiver in the emergency area for 72 hours beginning on implementation of a hospital disaster protocol. The waiver of HIPAA Privacy Rule requirements is effective only if actions under the waiver do not discriminate on the basis of a patient's source of payment or ability to pay. Also, the waiver only applies if the hospital has implemented its hospital disaster protocol. The HIPAA sanctions and penalties that may be waived when an 1135 waiver is issued are specified in the 1135 waiver document. An 1135 waiver does not waive HIPAA in its entirety. Even without an 1135 waiver, there are various flexibilities and exceptions that may apply to permit covered entities to share protected health information during a PHE.
Please see Disclosure for Emergency Preparedness for more information about the application of HIPAA during public health emergencies (whether or not the Secretary makes a formal PHE declaration under section 319 of the PHS Act, or issues an 1135 waiver).
Waivers or modifications under section 1135 of the SSA may be retroactive to the beginning of the emergency period (or to any subsequent date). The waiver or modification terminates either upon termination of the emergency period or 60 days after the waiver or modification is first published (subject to 60-day renewal periods until termination of the emergency). However, waivers of EMTALA (except in the case of a pandemic disease) or HIPAA requirements are effective only for 72 hours beginning on implementation of a hospital disaster protocol. A waiver of EMTALA sanctions in connection with an emergency involving a pandemic disease (such as pandemic influenza) is effective until the termination of the pandemic-related public health emergency. However, a particular waiver or modification will terminate prior to the ultimate termination date described in this paragraph (e.g., prior to the 72 hour time period after a hospital begins to implement its disaster protocol) if the Secretary determines that as of an earlier date, the waiver or modification is no longer necessary to accomplish the purposes set forth in Section 1135(a).
A PHE declaration lasts until the Secretary declares that the PHE no longer exists or upon the expiration of the 90-day period beginning on the date the Secretary declared a PHE exists, whichever occurs first. The Secretary may extend the PHE declaration for subsequent 90-day periods for as long as the PHE continues to exist, and may terminate the declaration whenever he determines that the PHE has ceased to exist.
Even without a PHE declaration, the Secretary has broad legal authority to provide assistance to states and to conduct research studies. For example, under section 301 of the PHS Act, the Secretary has broad authority to render assistance and promote research, investigations, demonstrations, and studies into the causes, diagnosis, treatment, control, and prevention of physical and mental diseases and impairments of man. Similarly, under section 311 of the PHS Act, the Secretary is authorized to assist states and their political subdivisions in the prevention and suppression of communicable diseases and to develop (and take necessary actions to implement) a plan under which personnel, equipment, medical supplies, and other resources of the Public Health Service and other agencies under the jurisdiction of the Secretary may be effectively used to control the epidemics of any disease or condition and to meet other health emergencies or problems. The Secretary may also activate the National Disaster Medical System under section 2812 of the PHS Act and deploy the Strategic National Stockpile under section 319F-2 of the PHS Act without a PHE declaration. For more information on actions the Secretary can take without a PHE declaration, see (insert link to page list the Secretary's authority when he has not declared a PHE).
No, a PHE declaration does not waive or preempt state licensing requirements. States determine whether and under what circumstances a non-federal healthcare provider is authorized to provide services in the state without state licensure.
As discussed in response #4 above, when the Secretary issues an 1135 waiver, the Secretary may waive Medicare, Medicaid, or CHIP requirements that physicians and other health care professionals hold licenses in the State in which they provide services. This would be for Medicare, Medicaid, or CHIP reimbursement purposes only, and would apply only if the physicians or other health care providers have an equivalent license from another state (and are not affirmatively barred from practice in any state in the emergency area).
No, a PHE declaration is not needed for the Secretary to authorize emergency use of medical countermeasures. The Secretary must issue a different declaration to authorize the Federal Food and Drug Administration to issue an Emergency Use Authorization (EUA) for an unapproved drug, biological product, or device or unapproved use of a drug, biological product, or device. The Secretary must declare that the emergency circumstances justify such authorization based on one of the following:
A determination by the Secretary of Homeland Security that there is an actual or significant potential for a domestic emergency involving a heightened risk of attack with a biological, chemical, radiological, or nuclear agent(s);
A determination by the Secretary of Homeland Security of a material threat of a chemical, biological, radiological, or nuclear agent sufficient to affect national security or the health and security of United States citizens living abroad.
A determination by the Secretary of Defense that there is a military emergency, or a significant potential for a military emergency, involving a heightened risk to United States military forces, including personnel operating under the authority of title 10 or title 50, of attack with (i) a biological, chemical, radiological, or nuclear agent or agents; or (ii) an agent or agents that may cause, or are otherwise associated with, an imminently life-threatening and specific risk to United States military forces.
His own determination that there is a public health emergency, or a significant potential for a public health emergency that affects, or has significant potential to affect, national security or the health and security of U.S. citizens living abroad and involves a biological, chemical, radiological, or nuclear agent(s) or a disease or condition that may be attributable to such agent(s).
No, under the PREP Act, codified at sections 319F-3 and 319F-4 of the PHS Act,, the Secretary may issue a declaration that provides liability immunity (except for willful misconduct) for claims of loss caused, arising out of, relating to, or resulting from administration and use of countermeasures to diseases, threats, and conditions determined by the Secretary to constitute a present or credible risk of a future public health emergency to entities and individuals involved in the development, manufacture, testing, distribution, administration, and use of such countermeasures.
A PREP Act declaration is different from a PHE. The declarations are made on different public health determinations and have different legal effects. A PREP Act Declaration may be made in advance of a public health emergency and may provide liability immunity for activities both before and after a declared public health emergency. A separate declaration under section 319 or other statutes is not needed for immunity under the PREP Act to take effect unless the PREP Act declaration states that a public health or other emergency declaration is needed to trigger immunity. For more information about the PREP Act, please see Public Readiness and Emergency Preparedness Q&As.
No, there is no requirement under section 319 of the PHS Act, nor under section 1135 of the SSA that a state or other entity make a formal request for a PHE declaration or an 1135 waiver. When state or local officials believe that a PHE declaration and 1135 waivers are needed to assist the response to a particular event, HHS encourages them to work with the HHS Regional Emergency Coordinator at the HHS regional office in their area who can help facilitate the request. Hospitals, healthcare entities, and healthcare providers who have concerns about Medicare, Medicaid, and CHIP requirements should contact the CMS regional office in their area who can help address such concerns.
No, the statutory language in section 319(a) of the PHS Act does not address a "potential" or threat of a PHE. However, the Secretary has the discretion to determine that a disease or condition "presents" a PHE or a PHE otherwise exists, based on conditions that exist prior to the actual outbreak of disease or natural catastrophe. For example, the Secretary may declare a PHE based on emergency needs that exist preceding the outbreak of disease or in anticipation of a storm before a hurricane makes landfall.
The Secretary may determine that there is a significant potential for a PHE to access the Public Health Emergency Fund (when funds are so appropriated), and may enable the Centers for Disease Control and Prevention Director to access the Infectious Diseases Rapid Response Reserve Fund (when funds are so appropriated) as discussed under questions #1 and #2 above.
The Secretary may also determine that a disease or disorder, including a novel and emerging public health threat, is significantly likely to become a public health emergency for purposes of waiving the PRA, as discussed under question #2 above.
A PHE declaration under section 319 of the PHS Act and a Presidential declaration of an emergency or disaster under the Stafford Act are distinct and separate declarations. When an incident overwhelms or is anticipated to overwhelm state or tribal resources, the Governor of an affected state or a Chief Executive of an affected Indian tribe, may request federal assistance, including assistance under the Stafford Act. The Stafford Act authorizes the President to provide financial and other assistance to state, local, and tribal governments, certain private nonprofit organizations, and individuals to support response, recovery, and mitigation efforts following Presidential emergency or disaster declarations.
The Stafford Act is triggered by a Presidential declaration of a major disaster or emergency, when an event causes damages of sufficient severity and magnitude to warrant federal disaster assistance to supplement the efforts and available resources of states, local, and tribal governments, and the disaster relief organizations in alleviating the damage, loss, hardship, or suffering. Most incidents are not of sufficient magnitude to warrant a Presidential declaration. However, if state and local resources are insufficient, a Governor or Chief Executive of an affected Indian tribe may ask the President to make such a declaration. Ordinarily only a Governor or a Chief Executive of an affected Indian tribe can initiate a request for a Presidential emergency or major disaster declaration. In extraordinary circumstances, the President may unilaterally declare an emergency.
Unlike a Presidential declaration of a major disaster or emergency under the Stafford Act which ordinarily requires a formal request by a state Governor or a Chief Executive of an affected Indian tribe, there is no requirement that a Governor, Chief Executive of an affected Indian tribe, or other entity make a formal request in order for the Secretary to declare a PHE under section 319 of the PHS Act. The President may declare a major disaster or emergency under the Stafford Act in the absence of a Secretarial declaration of a PHE under section 319 of the PHS Act. Likewise, the Secretary of HHS may declare a PHE under section 319 of the PHS Act in the absence of a Presidential declaration under the Stafford Act.
While a Presidential declaration under the Stafford Act and a Secretarial declaration of a PHE are separate declarations, sometimes a Stafford Act declaration is required in order for the Secretary to exercise certain authorities. For example, as discussed in the response to item #3 above, in order for the Secretary to exercise his waiver authority under section 1135 of the SSA to temporarily waive or modify certain Medicare, Medicaid, CHIP, and HIPAA Privacy Rule requirements, there must be a PHE declaration in place, as well as a Presidential declaration of a major disaster or emergency pursuant to the Stafford Act (or the National Emergencies Act).
Overview, Key Definitions, and DPA-related Executive Orders
The Defense Production Act (DPA) of 1950 is the primary source of Presidential authorities to expedite and expand the supply of materials and services from the U.S. industrial base needed to promote the national defense.
Since 1950, the DPA has been reauthorized more than 50 times, with Congress subsequently expanding the term national defense, as defined by the DPA, to include emergency preparedness activities conducted pursuant to title VI of the Stafford Act and critical infrastructure protection and restoration. The most recent reauthorization of the DPA extended the non-permanent provision of the act by six years, from September 30, 2019, to September 30, 2025 (Section 1791 of the John S. McCain National Defense Authorization Act for Fiscal Year 2019).
Defense Production Act Authorities
Current DPA authorities include:
Title I (Priorities and Allocations) allows the President to require businesses, corporations, and individuals to accept and prioritize contracts for materials and services necessary to promote the national defense and to allocate materials, services, and facilities necessary to promote the national defense.
Title III (Expansion of Productive Capacity and Supply) allows the President to incentivize the domestic industrial base expansion for the production and supply of critical materials and goods with specific limitations and requirements.
Title VII (General Provisions) includes key definitions for the DPA and authorities to:
Establish voluntary agreements with private industry,
Obtain information from businesses for industry studies,
Review proposed or pending foreign corporate mergers, acquisitions, or takeovers that threaten national security, and
Employ persons with recognized experience and establish a volunteer pool of industry executives who could be called to government service in the interest of the national defense.
Key Definitions
National defense: Programs for military and energy production or construction, military or critical infrastructure assistance to any foreign nation, homeland security, stockpiling, space, and any directly related activity. Such term includes emergency preparedness activities conducted pursuant to title VI of The Robert T. Stafford Disaster Relief and Emergency Assistance Act and critical infrastructure protection and restoration (DPA Sec. 702).
Emergency preparedness: All those activities and measures designed or undertaken to prepare for or minimize the effects of a hazard upon the civilian population, to deal with the immediate emergency conditions which would be created by the hazard, and to effectuate emergency repairs to, or the emergency restoration of, vital utilities and facilities destroyed or damaged by the hazard (full definition can be found in the Stafford Act Sec. 602).
Health resources: Drugs, biological products, medical devices, materials, facilities, health supplies, services, and equipment required to diagnose, mitigate or prevent the impairment of, improve, treat, cure, or restore the physical or mental health conditions of the population (EO 13603).
Critical infrastructure: Any systems and assets, whether physical or cyber-based, so vital to the United States that the degradation or destruction of such systems and assets would have a debilitating impact on national security, including, but not limited to, national economic security and national public health or safety (DPA Sec. 702).
DPA-Related Executive Orders
13603 National Defense Resources Preparedness Delegates DPA Title I, Title III, and Title VII authorities to agency heads. It specifies that Title I authorities "may be used only to support programs that have been determined in writing as necessary or appropriate to promote the national defense" by specific agency heads. The Secretary of Homeland Security will make determinations related to national defense programs, including civil defense and continuity of Government, not under the purview of the Secretary of Defense and the Secretary of Energy.
14001 A Sustainable Public Health Supply Chain Directed the HHS, DHS, DoD, and State secretaries to: (1) review and assess availability of "critical materials, treatments, and supplies" to combat COVID-19, (2) examine how DPA and other emergency authorities could address shortfalls, and (3) use DPA authorities as necessary for PPE and vaccines.
14017 America's Supply Chains Directed agency heads and the Assistant to the President for National Security Affairs (APNSA) and the Assistant to the President for Economic Policy (APEP) to: (1) review supply chain risks and submit a report to the President within 100 days and (2) in addition to reports from other agencies, HHS will submit a report on supply chains for the public health and biological preparedness industrial base within 1 year. Progress in implementation of issues related to public health is summarized in the Public Health Supply Chain and Industrial Base One-Year Report.
Contact Us
For more information about the Defense Production Act (DPA), please contact the HHS ASPR DPA Mailbox at aspr.dpa@hhs.gov
The Pandemic and All Hazards Preparedness Reauthorization Act amended section 564 of the Federal Food, Drug and Cosmetic (FD&C) Act, 21 U.S.C. 360bbb-3, to provide more flexibility to the Health and Human Services Secretary to authorize the U.S.